
Vasectomy
Overview
A vasectomy is a safe, easily performed outpatient procedure that provides an effective, permanent form of birth control for men. You should not have a vasectomy unless you and your partner are sure you do not wish to have children in the future.
Many men understandably have fears about a procedure involving their scrotum. The good news is that a vasectomy has absolutely no effect on a man’s masculinity, sex drive, ejaculation, ability to have an erection or sexual pleasure.
There is little pain or discomfort during or after the procedure. Some urologists perform a “no scalpel” vasectomy, which uses a small puncture instead of a cut and which may result in less pain and swelling. Both the traditional method and this method are safe and effective.
If you have any fears or questions, don’t hesitate to talk about them with your urologist.
Why Have A Vasectomy
Vasectomy should be considered a permanent form of sterilization. It is a completely elective operative procedure. It is not an appropriate option for patients who might consider starting a new family or having additional children in the future should their social situations change. The decision to have a vasectomy should be made only after careful consideration regarding the possibility of wanting to have additional children in the future. The decision to have a vasectomy should almost always be made after discussion with the patient’s partner. The patient considering a vasectomy should also consider the risks and side effects of an unwanted pregnancy. While there are many other ways to prevent pregnancy, vasectomy is one of the most reliable ways to permanently prevent pregnancy. It requires less expense and is much safer than tubal ligation in women.
History of the Vasectomy Procedure
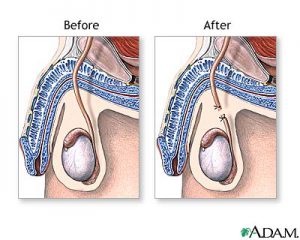
Vasectomy has been performed in the United States for decades. In 1974 a Chinese surgeon developed the “no scalpel” vasectomy technique. This technique was brought to the United States in 1985. The no scalpel technique is performed by many of our urologists. It seems to provide advantages over conventional vasectomy by reducing the operative time, and decreasing risks of bleeding and discomfort. It is just as effective as a conventional vasectomy. Sperm is produced by both testicles. The sperm leaves the testicle near the upper pole and enters a structure called the epididymis. Inside the epididymis is an 18 ft. long delicate coiled tube that the sperm travel through. The epididymal tube then empties into the vas deferens which is a thick cord-like structure that can be felt within the scrotum. The vas deferens tube travels up through the scrotum into the inguinal canal and dives deep into the pelvis behind the bladder and prostate. When a man has an orgasm, fluid from the seminal vesicles and prostate mix with the sperm and the combination of this fluid becomes the ejaculate. A vasectomy is performed by removing a section of the vas deferens tube within the scrotum to prevent sperm from being transported from the testicle to the ejaculatory duct area. The tubes from both right and left sides are accessed through the wall of the scrotum and a section is removed. The ends of the vas deferens are then occluded by a choice of several techniques. Some surgeons use sutures or clips, but most physicians use cautery or heat to seal the ends closed.
The Vasectomy Procedure
The vasectomy is performed in the office by the urologist. It is performed under local anesthetic injected through a tiny needle into the skin. For patients who are extremely nervous or anxious, oral sedation is sometimes prescribed at the time of the initial office consultation. The hair may be shaved from the scrotum, and the skin is prepared with an antiseptic. With the conventional vasectomy, one or two scrotal incisions are made with a scalpel and the vas deferens is visualized and a section is cut and removed from both sides. The ends are occluded according to the surgeon’s preferred technique. Generally, absorbable sutures are used to close the skin at the conclusion of the procedure. Most urologists have the patient bring a jock strap to hold the dressing in place and provide support for the scrotum for several days. With the no scalpel vasectomy technique, a single puncture is made in the middle of the scrotal skin and the skin is stretched open about 4 mm. A special clamp is then used to grasp the vas deferens and bring it out above the skin. The rest of the procedure is then performed above the level of the skin. Both sides can be done through a single puncture site. The puncture site is so small that sutures are not routinely used. The puncture site generally heals in one or two days. Some urologists perform open ended vasectomies. The abdominal end of the vas deferens is sealed but the testicular end is left open to prevent pressure induced damage to the epididymis which may decrease the potential long-term complications of chronic epididymal pain.
A vasectomy is a surgical procedure, and therefore has potential side effects. The short-term effects of vasectomy are primarily bleeding within the scrotum, bruising, infection, and discomfort. Infection is very rare. Bruising of the scrotal wall is common but rarely causes pain or discomfort. The primary serious short-term side effect of a vasectomy is the risk of formation of scrotal hematoma. This occurs in about 0.5 – 1 percent of patients undergoing vasectomy in the hands of an experienced urologist. The scrotum is a unique part of the body which will expand under increasing volume allowing bleeding to continue. It is extremely important, therefore, for the patient to carefully follow the instructions of the urologist in the postoperative period to avoid hematoma formation by resuming activities too soon. Hematomas cause significant scrotal pain, but rarely require additional surgery. The long-term side effects of vasectomy include inability to father children, which is the intended effect of the vasectomy procedure. In addition, chronic epididymal pain can occur in 2 – 4 percent of patients due to pressure-induced swelling of the epididymis. This can usually be treated with over the counter nonsteroidal anti-inflammatory drugs such as ibuprofen. Sperm granuloma formation is common and is usually asymptomatic if it occurs at the cut end of the vas deferens In the mid-1990’s, an article was published which suggested the possibilty that having a vasectomy could increase of patient’s risk of getting prostate cancer later in life. Multiple studies have since been undertaken which have failed to show a clear link between vasectomy and an increased risk of prostate cancer. The vast majority of scientific evidence finds that vasectomy does not lead to any form of chronic disease, coronary disease, or in the increased risk of cancer.
After Surgery
Patients who are considering a vasectomy should plan on very limited physical activity for two or three days after the procedure is performed. Patients who do primarily office work can usually have the procedure performed on Firday and return to work on Monday. Patients whose jobs involve heavy lifting or strenuous activity, such as firefighters or construction workers, should probably take a few days off of work after a vasectomy. It is very important that the patients avoid any form of strenuous exercise or heavy lifting for five to seven days after the procedure. This is to insure that the patient does not develop delayed bleeding with formation of scrotal hematoma. Most patients can resume full activities, including sexual activity, about seven days after the procedure.
The patient is not sterile immediately after the procedure. It takes approximately 15 ejaculations and several weeks for all of the sperm to be washed out of the ductal system. During this time, it is quite possible to cause a pregnancy. Alternative forms of birth control must continue to be used during this time. After 15 ejaculations, the patient is asked to bring in a fresh sample of semen for evaluation by the surgeon. This sample should have no sperm in it under microscopic examination. If no sperm are seen, the patient is considered sterile. If any sperm are seen, the patient is warned to continue using an alternative form of birth control and resubmit a semen sample after 10 additional ejaculations. A second semen sample is required within one to six months to insure that recanalization has not occurred during the healing process. Once the second semen sample is found to be free of sperm, the patient can expect to be permanently sterile.
Considerations
The success of vasectomy is not 100 percent. Approximately 1 in 200-400 patients who undergo vasectomy will not have sperm permanently removed from their ejaculate. To put this in to perspective, the failure rate of preventing pregnancy with condoms is approximately 30 percent. Birth control pills and long-term hormone shots are about 97-98 percent effective at preventing pregnancy when used appropriately. Tubal ligation has a failure rate of approximately 1 percent, and when tubal ligation does fail, the mother is at increased risk of a tubal pregnancy. Tubal pregnancies have significant potential complications including death. Vasectomies appear to be more than 99 percent effective at preventing pregnancy. The only more reliable way to prevent pregnancy is to completely abstain from sexual activity.
If you are interested in learning more about vasectomy, please call our office to schedule an appointment with one of our physicians. Some ot the urologists require a consultation at the office prior to scheduling a vasectomy. This ensures that all of your questions will be answered, that your examination is normal, and that you are a good candidate for vasectomy.


