
Benign Prostatic Hyperplasia (BPH)
Overview
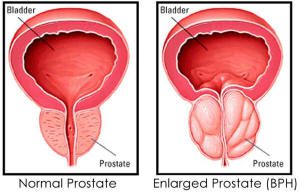
Benign Prostatic Hyperplasia (BPH) is a common, benign (non cancerous) condition in older men in which you see a enlarged prostate. The prostate is a walnut-sized gland that produces semen, the fluid that transports sperm. Located in front of the rectum and just below the bladder, where urine is stored, the prostate surrounds the urethra (the tube carrying urine out of the body). The enlarged prostate squeezes the urethra causing difficulty with urination.
The cause of BPH is not well understood. No definite information on risk factors exists. For centuries, it has been known that BPH occurs mainly in older men and that it doesn’t develop in men whose testes were removed before puberty. For this reason, some researchers believe that factors related to aging and the testes may spur the deveopment of BPH.
Throughout their lives, men produce both testosterone, an important male hormone, and small amounts of estrogen, a female hormone. As men age, the amount of active testosterone in the blood decreases, leaving a higher proportion of estrogen. Studies done on animals have suggested that BPH may occur because the higher amount of estrogen within the gland increases the activity of substances that promote cell growth.
Symptoms
BPH rarely causes symptoms before age 40, but more than half of men in their sixties and as many as 90 percent in their seventies and eighties have some symptoms of BPH. Many symptoms of BPH stem from obstruction of the urethra and gradual loss of bladder function, which results in incomplete emptying of the bladder. The symptoms of BPH vary, but most common ones involve changes or problems with urination, such as:
- Recurring, sudden need to urinate
- Increasingly frequent urination, especially at night
- Weak or interrupted urine stream
- Difficulty starting urination
- Urine leakage
- Inability to completely empty the bladder
- Blood in the urine (hematuria)
The size of the prostate does not always determine how severe the obstruction or the symptoms will be. Some men with greatly enlarged glands have little obstruction and few symptoms while others, whose glands are less enlarged, have more blockage and greater problems.
Sometimes a man may not know he has any obstruction until he suddenly finds himself unable to urinate at all. This condition, called acute urinary retention, may be triggered by taking over-the-counter cold or allergy medicines. Such medicines contain a decongestant drug, known as a sympathomonimetic. A potential side effect of this drug may prevent the bladder opening from relaxing and allowing urine to empty. When partial obstruction is present, urinary retention also can be brought on by alcohol, cold temperatures, or a long period of immobility.
It is important to tell your doctor about urinary problems such as those described above. In eight out of 10 cases, these symptoms suggest BPH, but they also can signal other, more serious conditions that require prompt treatment. These conditions, including prostate cancer, can be ruled out only by a doctor’s examination.
Severe BPH can cause serious problems over time. Urine retention and strain on the bladder can lead to urinary tract infections, bladder or kidney damage, bladder stones, and incontinence–the inability to control urination. If the bladder is permanently damaged, treatment for BPH may be ineffective. When BPH is found in its earlier stages, there is a lower risk of developing such complications.
Diagnosis
You may first notice symptoms of BPH yourself, or your doctor may find that your prostate is enlarged during a routine checkup. When BPH is suspected, you may be referred to a urologist, a doctor who specializes in problems of the urinary tract and the male reproductive system. Several tests help the doctor identify the problem and decide whether surgery is needed. The tests vary from patient to patient, but the following are the most common.
Digital Rectal Examination (DRE) – This examination is usually the first test done. The doctor inserts a gloved finger into the rectum and feels the part of the prostate next to the rectum. This examination gives the doctor a general idea of the size of the gland.
Prostate-Specific Antigen (PSA) Blood Test – To rule out cancer as a cause of urinary symptoms, your doctor may recommend a PSA blood test. PSA, a protein produced by prostate cells, is frequently present at elevated levels in the blood of men who have prostate cancer. The U.S. Food and Drug Administration (FDA) has approved a PSA test for use in conjunction with a digital rectal examination to help detect prostate cancer in men who are age 50 or older and for monitoring men with prostate cancer after treatment. However, much remains unknown about the interpretation of PSA levels, the test’s ability to discriminate cancer from benign prostate conditions, and the best course of action following a finding of elevated PSA. While the normal range should be less than 4.0, younger men should have a PSA that is less than 2.5.
Trans-Rectal Ultrasound -If there is a suspicion of prostate cancer, your doctor may recommend a test with rectal ultrasound. In this procedure, a probe inserted in the rectum directs sound waves at the prostate. The echo patterns of the sound waves form an image of the prostate gland on a display screen. To determine whether an abnormal-looking area is indeed a tumor, the doctor can use the probe and the ultrasound images to guide a biopsy needle to the suspected tumor. The needle collects a few pieces of prostate tissue for examination with a microscope. If biopsies are taken, the prostate is injected with numbing medication first and the biopsies are taken after the medication has taken effect, thus causing minimal discomfort.
Urine Flow Study – Sometimes your physician at Florida Urology may ask you to urinate into a special device that measures how quickly the urine is flowing. A reduced flow often suggests BPH.
Cystoscopy – In this examination, the doctor inserts a small tube through the opening of the urethra in the penis. This procedure is done after a solution numbs the inside of the penis so all sensation is lost. The tube, called a cystoscope, contains a lens and a light system that help the doctor see inside of the urethra and the bladder. This test allows the doctor to determine the size of the gland and identify the location and degree of the obstruction.
Treatments
There are several treatment options for men with benign prostatic hyperplasia, depending on the severity of symptoms. If symptoms do not threaten the man’s health, he may choose not to be treated. If symptoms are severe enough to cause discomfort, interfere with daily activities, or threaten health, treatment is usually recommended.
WATCHFUL WAITING
Watchful waiting is recommended as an important option for men who have mild symptoms and do not find them particularly bothersome. It is the least invasive treatment and avoids the risks, inconvenience and costs of medical and surgical treatments. In some men, symptoms improve over time as long as there are no high-risk symptoms like urinary retention, recurrent urinary tract infection, recurrent blood in the urine, bladder stones, kidney failure or bladdder diverticula.
DRUG TREATMENT
Alpha Blockers – These drugs, originally used to treat high blood pressure, work by relaxing the smooth muscle of the prostate and bladder neck to improve urine flow and reduce bladder outlet obstruction. Although alpha blockers may relieve the symptoms of BPH, they usually do not reduce the size of the prostate. They are usually taken orally, once or twice a day just before bedtime and they work almost immediately. Commonly prescribed alpha blockers include: terazosin, doxazosin and tamsulosin. Side effects can include headaches, dizziness, light-headiness, fatigue and difficulty breathing.
5-Alpha Reductase Inhibitors – Finasteride is an oral medication that works completely different then alpha blockers. In some men, finasteride can relieve BPH symptoms, increase urinary flow rate and actually shrink the prostate though it must be used indefinitely to prevent recurrence of symptoms. One study suggests that finasteride may be best suited for men with relatively large prostate glands. It may take as long as six months to a year, however, to achieve maximum benefits from this drug. Side effects can include impotence, decreased libido and reduced semen release during ejaculation.
MINIMALLY INVASIVE TREATMENTS
Transurethral Electroevaporation of the Prostate (TUVP) – After the patient receives anesthesia, the surgeon inserts an instrument called a resectoscope through the penis into the urethra. The resectoscope contains a light, valves for controlling irrigating fluid and a grooved rolling metal electrode. This electrode moves across the surface of the prostate and electrical current vaporizes prostate tissue. The vaporizing effect penetrates below the surface area being treated so underlying blood vessels are coagulated and sealed. Bleeding and fluid absorption are minimal and patients can usually return home without a catheter after an overnight hospital stay.
Transurethral Microwave Thermotherapy of the Prostate (TUMT) – This is an office-based procedure performed with topical and oral pain medication and does not require anesthesia. Computer-regulated microwaves are sent through a catheter to heat portions of the prostate. A cooling system works simultaneously to protect the urinary tract during the procedure. Traditionally, the best use of this procedure has been for patients who have too many medical problems for more invasive surgery or for patients who truly wish to avoid any type of anesthesia. Benefits are that there is no need for anesthesia and there is no blood loss or fluid absorption (these would be significant benefits in a person with a weak heart). Patients usually go home the same day. Many urologists have the technology available in their practice and results are pretty reliable regardless of who performs the procedure. The use of TUMT has been expanding to a broader patient population.
GreenLight PVP – The GreenLight PVP Laser Procedure (Photoselective Vaporization of the Prostate) offers a unique and simple solution to BPH because it combines the effectiveness of TURP, the surgical “gold standard” with the safety, comfort and ease of a minimally invasive treatment. The GreenLight PVP Laser Procedure uses a very high-powered laser to immediately vaporize and precisely remove enlarged prostate tissue. Most patients return home a few short hours after the procedure and can return to normal, non-strenuous activities within days.
SURGERY
When medical therapy fails, surgery is required to remove the obstructing tissue. Surgery is usually recommended for men who are unable to urinate, have kidney damage, frequent urinary tract infections, significant urethral bleeding or stones in the bladder. Removal of the prostate can be accomplished in several different ways. The extent of the enlargement and the patient’s general health will determine which of the following procedures to use.
Transurethral Resection of the Propstate (TURP) – Transurethral resection of the prostate is a surgical procedure performed through the urethra to remove obstructing prostate tissue. While under anesthesia, an instrument called a resectoscope is inserted into the urethra and advanced to the prostate. The resectoscope contains a light, valves for controlling irrigating fluid and an electrical loop that cuts tissue and seals blood vessels. With this instrument, obstructive prostate tissue is removed one piece at a time. The removed tissue is sent for pathologic examination. At the end of the procedure, a catheter is placed in the bladder through the penis. The bladder is continuously irrigated with fluid through the catheter in order to monitor bleeding and prevent blood from clotting and obstructing the catheter. Since there are no surgical incisions with this procedure, patients normally stay in the hospital only one or two days.
Open Prostatectomy – When a transurethral procedure cannot be done, open surgery may be required. Open prostatectomy for BPH is also performed for a prostate that is too large to remove through the penis. Other reasons for choosing an open prostatectomy include patients with large bladder diverticula, with large bladder stones and who cannot physically tolerate having their legs placed in stirrups for TURP surgery. An incision is made in the abdominal wall from below the belly button to the pubic bone. The prostate gland can then be removed in its entirety through either an incision in the fibrous capsule surrounding the prostate (retropubic prostatectomy) or through an incision made in the bladder (suprapubic prostatectomy).
The amount of time you will stay in the hospital depends on the type of surgery you had and how quickly you recover. At the end of surgery, a special catheter is inserted through the opening of the penis to drain urine from the bladder into a collection bag. Called a Foley catheter, this device has a water-filled balloon on the end that is put in the bladder, which keeps it in place. This catheter is usually left in place for several days. Sometimes, the catheter causes recurring painful bladder spasms the day after surgery. These spasms may be difficult to control, but they will eventually disappear. You may also be given antibiotics while you are in the hospital. Many doctors start giving this medicine before or soon after surgery to prevent infection. However, some recent studies suggest that antibiotics may not be needed in every case, and your doctor may prefer to wait until an infection is present to give them. After surgery, you will probably notice some blood or clots in your urine as the wound starts to heal. If your bladder is being irrigated (flushed with water), you may notice that your urine becomes red once the irrigation is stopped. Some bleeding is normal, and it should clear up by the time you leave the hospital. During your recovery, it is important to drink a lot of water (up to 8 cups a day) to help flush out the bladder and speed healing.
Lifestyle Changes
- Avoid caffeine, acidic drinks such as colas, tomato and orange juice, and alcohol. Cold medications containing antihistamines or pseudoephedrin, and constipation can make it more difficult to urinate.
- Limit evening beverages and urinate when you first feel the urge.
- Increase your physical activity level.


